|
Oxytocin binds to G-protein coupled
receptors. In human myometrium these
receptors couple to Gq and G11
receptors. This will activate
Phospholipase -C hydrolysis and generate
Inositol triphosphate (IP3) and Diacyl
glycerol. These will mobilizes calcium
ion from calcium deposits and also
enhances voltage sensitive Ca2+
channels. This Ca2+ produces
contraction.
1. Induction of labour
2. Augmentation of labour
3. Reduction of postpartum bleeding
4. Induce abortion
5. Oxytocin challenge test
Copyright © 2004-2007 Taj Pharmaceuticals Ltd. All rights
reserved.This information is intended
only for residents of the India. Litocin
(Trademark Of Taj Pharmaceuticals Ltd.,
India)
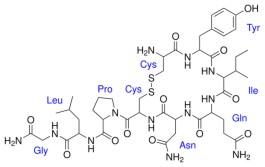
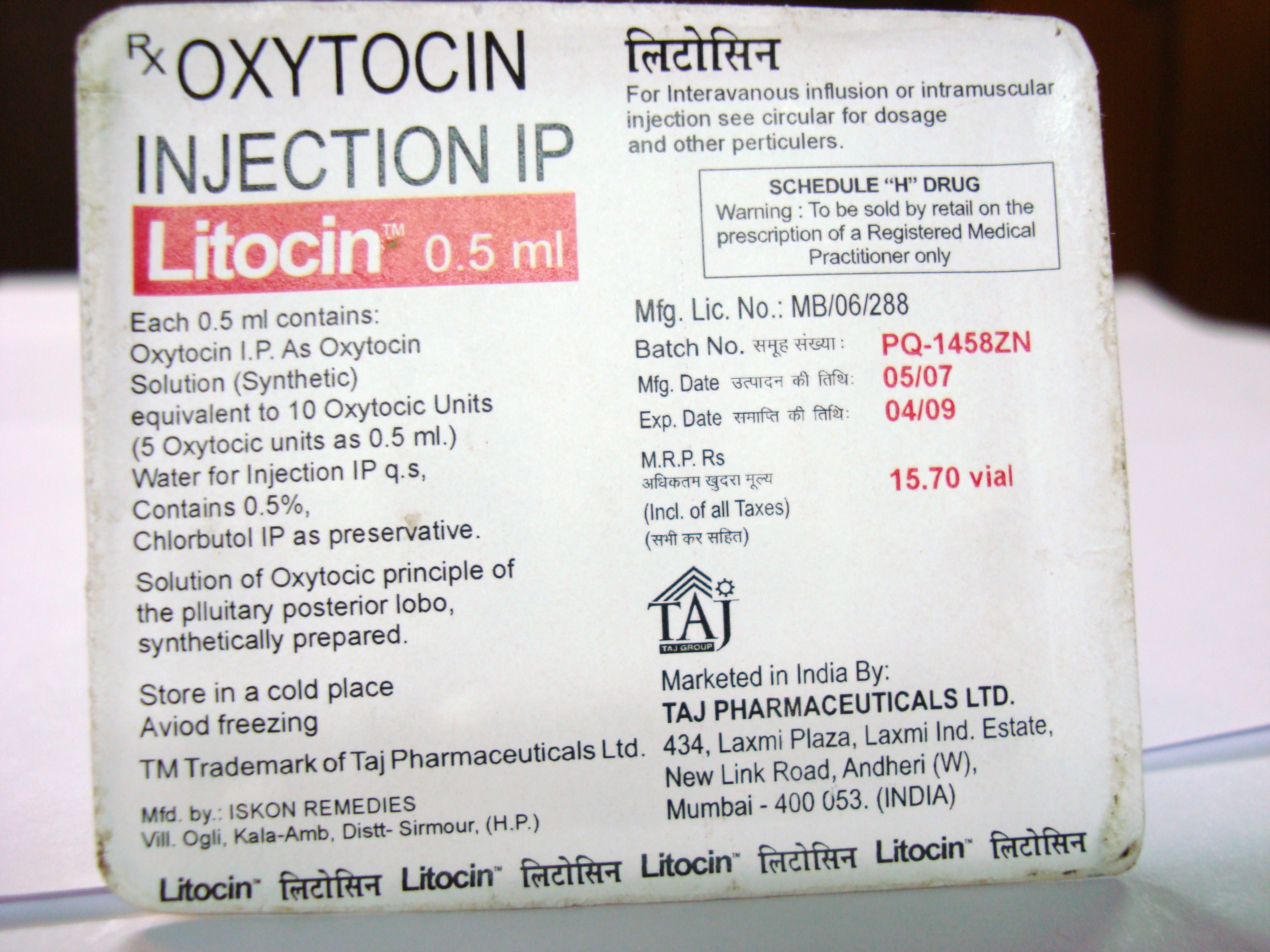
Litocin (oxytocin injection,USP) is a
sterile,clear,colorless aqueous solution
of synthetic oxytocin, for intravenous
infusion or intramuscular
injection.Litocin is a nonapeptide found
in pituitary extracts from mammals. It
is standardized to contain 10 units of
oxytocic hormone/mL and contains 0.5%
Chlorobutanol,a chloroform derivative as
a preservative,with the pH adjusted with
acetic acid. Litocin may contain up to
16% of total impurities.The hormone is
prepared synthetically to avoid possible
contamination with vasopressin (ADH) and
other small polypeptides with biologic
activity. Litocin has the empirical
formula C43H66N12O12S2 (molecular weight
1007.19).
IMPORTANT NOTICE :
Elective induction of labor is
defined as the initiation of labor in a
pregnant individual who has no medical
indications for induction. Since the
available data are inadequate to
evaluate the enefits-to-risks
considerations, Litocin is not indicated
for elective induction of labor.
Litocin is indicated for the initiation or improvement of uterine
contractions,where this is desirable and
considered suitable for reasons of fetal
or maternal concern, in order to achieve
vaginal delivery. It is indicated for
(1) induction of labor in patients with
a medical indication for the initiation
of labor,such as Rh problems, maternal
diabetes, preeclampsia at or near term,
when delivery is in the best interests
of mother and fetus or when membranes
are prematurely ruptured and delivery is
indicated;
(2) stimulation or reinforcement of
labor,as in selected cases of uterine
inertia;
(3) as adjunctive therapy in the management of incomplete or inevitable
abortion. In the first trimester,
curettage is generally considered
primary therapy.In second trimester
abortion, oxytocin infusion will often
be successful in emptying the uterus.
Other means of therapy,however,may be
required in such cases.
Postpartum: Litocin is indicated
to produce uterine contractions during
the third stage of labor and to control
postpartum bleeding or hemorrhage.
Parenteral drug products should be inspected visually for particulate
matter and discoloration prior to
administration whenever solution and
container permit.
The dosage of oxytocin is determined by
the uterine response and must therefore
be individualized and initiated at a
very low level. The following dosage
information is based upon various
regimens and indications in general use.
A. Induction or Stimulation of
Labor :
Intravenous infusion (drip method) is
the only acceptable method of parenteral
administration of Pitocin for the
induction or stimulation of labor.
Accurate control of the rate of infusion
is essential and is best accomplished by
an infusion pump. It is convenient to
piggyback the Pitocin infusion on a
physiologic electrolyte
solution,permitting the Pitocin infusion
to be stopped abruptly without
interrupting the electrolyte
infusion.This is done in the following
way.
1. Preparation :
a. The standard solution for infusion of
Litocin is prepared by adding the
contents of one 1-mL ampoule containing
10 units of oxytocin to 1000 mL of 0.9%
aqueous sodium chloride or Ringer’s
lactate. The combined solution
containing 10 milliunits (mU) of
oxytocin/mL is rotated in the infusion
bottle for thorough mixing.
b. Establish the infusion with a
separate bottle of physiologic
electrolyte solution not containing
Litocin.
c. Attach (piggyback) the Litocin-containing
bottle with the infusion pump to the
infusion line as close to the infusion
site as possible.
2. Administration :
The initial dose should be 0.5–1 mU/min
(equal to 3–6 mL of the dilute oxytocin
solution per hour). At 30–60 minute
intervals the dose should be gradually
increased in increments of 1–2 mU/min
until the desired contraction pattern
has been established.Once the desired
frequency of contractions has been
reached and labor has progressed to 5–6
cm dilation, the dose may be reduced by
similar increments.
Studies of the concentrations of
oxytocin in the maternal plasma during
Litocin infusion have shown that
infusion rates up to 6 mU/min give the
same oxytocin levels that are found in
spontaneous labor.At term, higher
infusion rates should be given with
great care,and rates exceeding 9–10 mU/min
are rarely required. Before term, when
the sensitivity of the uterus is lower
because of a lower concentration of
oxytocin receptors, a higher infusion
rate may be required.
3. Monitoring :
a. Electronically monitor the uterine
activity and the fetal heart rate
throughout the infusion of
Litocin.Attention should be given to
tonus, amplitude and frequency of
contractions, and to the fetal heart
rate in relation to uterine
contractions. If uterine contractions
become too powerful,the infusion can be
abruptly stopped,and oxytocic
stimulation of the uterine musculature
will soon wane (see PRECAUTIONS
section).
b. Discontinue the infusion of Litocin
immediately in the event of uterine
hyperactivity and/or fetal distress.
Administer oxygen to the mother, who
preferably should be put in a lateral
position. The condition of mother and
fetus should immediately be evaluated by
the responsible physician and
appropriate steps taken.
B. Control of Postpartum Uterine
Bleeding :
1. Intravenous infusion (drip method).If
the patient has an intravenous infusion
running,10 to 40 units of oxytocin may
be added to the bottle,depending on the
amount of electrolyte or dextrose
solution remaining (maximum 40 units to
1000 mL). Adjust the infusion rate to
sustain uterine contraction and control
uterine atony.
2. Intramuscular administration.(One mL)
Ten (10) units of Litocin can be given
after the delivery of the placenta.
C. Treatment of
Incomplete,Inevitable,or Elective
Abortion :
Intravenous infusion of 10 units of
Litocin added to 500 mL of a physiologic
saline solution or 5% dextrose-in-water
solution may help the uterus contract
after a suction or sharp curettage for
an incomplete, inevitable, or elective
abortion.
Subsequent to intra-amniotic injection
of hypertonic saline,
prostaglandins,urea,etc.,for
midtrimester elective abortion, the
injection-to-abortion time may be
shortened by infusion of Litocin at the
rate of 10 to 20 milliunits (20 to 40
drops) per minute.The total dose should
not exceed 30 units in a 12-hour period
due to the risk of water intoxication.
HOW SUPPLIED :
Litocin (Oxytocin Injection,USP)
Synthetic is available as follows:
LPT 61570-416-01 Packages of ten 1-mL
ampoules, each containing 10 units of
oxytocin.
LPT 61570-416-05 Packages of twenty-five
oversized 1-mL Steri-Vials, each
containing 10 units of oxytocin.
Intravenous or intramuscular Adult: 1.
Induction of labour: Initial dose: 0.5-
1 milliunits /minute as IV infusion and
if needed rate can be gradually
increased by 1 - 2 milliunits/minute
until sufficient response is obtained.
2. Augmentation of labour: Initial dose:
2milliunits/minute as intravenous
infusion and then gradually increase the
dose maximum up to 20milliunits/minute
3. Reduction of postpartum bleeding
after expulsion of placenta: 20 - 40
milliunits/minute as intravenous
infusion after delivery of placenta. 4.
Induce abortion: 10 - 100 milliunits/minutes
5. Oxytocin challenge test to assess
fetal distress in high risk pregnancies
greater than 31 weeks` gestation:
Initial dose: 0.5milliunits/minute
followed by gradual increase in infusion
rate every 15 minutes up to
20milliunits/minute. When 3 moderate
uterine contractions occur in a 10
minute interval then stop the use of
medicament.
Store at 2 - 8 degree C.
Manufactured and Distributed by:
Taj Pharmaceuticals Ltd,
India.,Mumbai,TN 37620 Reaserched by:
Parkedale
Pharmaceuticals,Inc.,Rochester,MI 48307
PACKAGING
INFORMATION
:
Injection 0.5 ml 0.5ml
Injection 1 ml 1ml
Wallpapers :


CLICK ON PHOTO TO SEE LARGE.
|



.JPG)